
Burn Classification & Assessment: Classification, Assessment & Initial Treatment
Burn injuries are medical emergencies that require prompt evaluation and structured management. Effective treatment depends on early assessment of burn severity, depth, and extent. A systematic approach ensures that life-threatening complications are managed immediately while planning definitive care. Understanding burn classification and assessment is essential for accurate diagnosis, proper intervention, and improved patient prognosis.
Initial Protocol for Burn Patients
Upon arrival, a set protocol guides the assessment, analysis, and treatment of burn patients. This systematic approach ensures all critical aspects are addressed efficiently.
Primary Survey in Burns Management
The initial and most crucial step is performing a primary survey using the ABCDE approach. This aims to rule out any immediate life-threatening injuries. The components are:
-
Airway with Cervical spine stabilization
-
Breathing with Ventilation
-
Circulation and Hemorrhage control
-
Disability limitation
-
Expose and examine
Immediate Interventions During Primary Survey for Burns
During the primary survey, specific interventions are immediately initiated for burn patients:
-
Oxygen Administration: Place a face mask and administer 100% oxygen. This is crucial due to potential inhalational burns or fumes causing airway damage.
-
Intravenous Access: Secure two large IV cannulas. 16 gauge is preferred over 18 gauge for significant burns.
-
Tetanus Prophylaxis: Administer 0.5 cc intramuscular tetanus toxoid (TT) as a prophylactic measure.
Warning Signs for Intubation in Burn Patients
It is critical to look for warning signs that necessitate immediate intubation in a burn patient. If any of these are present, the patient must be intubated immediately:
-
Presence of hoarseness of voice (suggesting laryngeal edema due to inhalational burns).
-
Presence of inspiratory stridor.
-
Evidence of facial burns.
-
Presence of severe wheezing on auscultation.
Read more: Trauma & ATLS Protocol
Secondary Survey in Burns Management
After the primary survey, proceed to the secondary survey to rule out any potentially life-threatening injuries. The primary goal for burn patients during this survey is the assessment of the extent of the burn, determining decisions for patient admission or transfer to a burn unit. This assessment of the extent/percentage of body surface area burnt is evaluated during the secondary survey.
Defining Significant vs. Insignificant Burns
The assessment classifies burns as significant or insignificant:
-
Significant Burn: Total body surface area (TBSA) burnt is more than 15%.
-
Management: Requires resuscitation, with Ringer's lactate as the fluid of choice. A Foley catheter is deployed to measure urine output to assess resuscitation response. Wound care management is also critical.
-
Insignificant Burn: Total body surface area (TBSA) burnt is less than 15%.
-
Management: Involves local management, primarily basic wound care and moist dressings.
Wound Irrigation and Debridement
Regardless of the burn's significance, wound irrigation and debridement must be performed.
Viable vs. Non-viable Tissue Management
Following debridement, tissue viability is assessed:
-
Non-viable tissue: Requires skin grafting or flap reconstruction.
-
Viable tissue: Managed with local burn wound care using topical agents and dressings.
Burn Management Algorithm
The overall algorithm for managing burn patients in casualty involves:
-
Primary Survey (ABCDE).
-
Immediate Interventions: Oxygenation (100% O2 via mask), securing two large IV cannulas, and administering tetanus toxoid.
-
Monitoring for warning signs for intubation.
-
Secondary Survey: Assessing for significant or insignificant burns.
-
Wound Management: Includes assessing the extent of the burn and initiating resuscitation protocols as needed. Maintaining oxygenation and secure IV lines is essential for patient stability.
Read More: Traumatic Brain Injury
Burn Wound Management: Thorough Wash
A crucial step in burn wound management is providing a thorough wash.
-
Objective: The primary objective is not to sterilize the wound, but to provide a cool-down effect, preventing further heat dissipation into deeper tissues.
-
Preferred Fluid: Tap water at room temperature is suitable (Memory Tip: While European room temperature is considered 15°C, 20-25°C is acceptable in the Asian subcontinent. The core concept is achieving a cool-down effect.).
-
Duration: The wash should be run for 15 to 20 minutes. Prolonged washing can lead to hypothermia.
-
Effectiveness Window: This intervention is only effective if the patient presents within 1 hour of the burn. After 1 hour, it becomes ineffective as tissue damage is already established.
Criteria for Admission in a Burn Ward
Admission to a burn ward is indicated if a patient cannot be safely managed at home. Specific criteria for admission include:
-
Suspected inhalational injury.
-
Requirement for fluid resuscitation.
-
Requirement for any form of surgery.
-
Burns on notorious sites: Hands, feet, and perineum.
-
Psychiatric illness or poor social background.
-
Suspicion of non-accidental burn.
-
Burns in extreme of age:
-
Age less than 10 years.
-
Age above 50 years.
-
Burns associated with potentially serious sequelae:
-
Electrical burns.
-
Alkali burns.
-
Acid burns.
Assessment of Total Body Surface Area (TBSA) Burnt
Assessing the total body surface area (TBSA) burnt is a critical step.
-
The most commonly used rule for TBSA assessment is the Valis rule, also known as the Rule of Nine.
-
The best method for TBSA assessment is the Lund and Browder's chart.
Rule of Nine (Valis Rule) for TBSA Assessment
The Valis rule (Rule of Nine) is a frequently tested concept, differing for adults and children:
|
Rule of Nine (Valis Rule) for TBSA Assessment |
||
|---|---|---|
|
Body Part |
Adult Percentage (Each Side/Limb) |
Child Percentage (Each Side/Limb) |
|
Head and Neck |
9% |
18% |
|
Trunk Anterior |
18% |
18% |
|
Trunk Posterior |
18% |
18% |
|
Upper Limb |
9% |
9% |
|
Palm (alone) |
1% |
1% |
|
Perineum |
1% |
Not considered |
|
Lower Limb |
18% |
14% |
(Memory Tip: In adults, head and neck is 9%, lower limb is 18%. In children, head and neck is 18%, lower limb is 14%. Perineum is not separately counted in children.)
Also Read: CNS Physiology MBBS 1st Year
Definition of Significant Burn (Age-Based & Uniform)
The definition of a significant burn also depends on the age of presentation:
|
Rule of Nine (Valis Rule) for TBSA Assessment |
|
|---|---|
|
Age Group |
Criteria for Significant Burn (TBSA) |
|
Less than 10 years |
≥ 10% |
|
10 to 50 years |
≥ 20% |
|
Above 50 years |
≥ 10% |
To avoid confusion, if age-specific data is not requested, a uniform definition for significant burn across all ages is ≥ 15% TBSA.
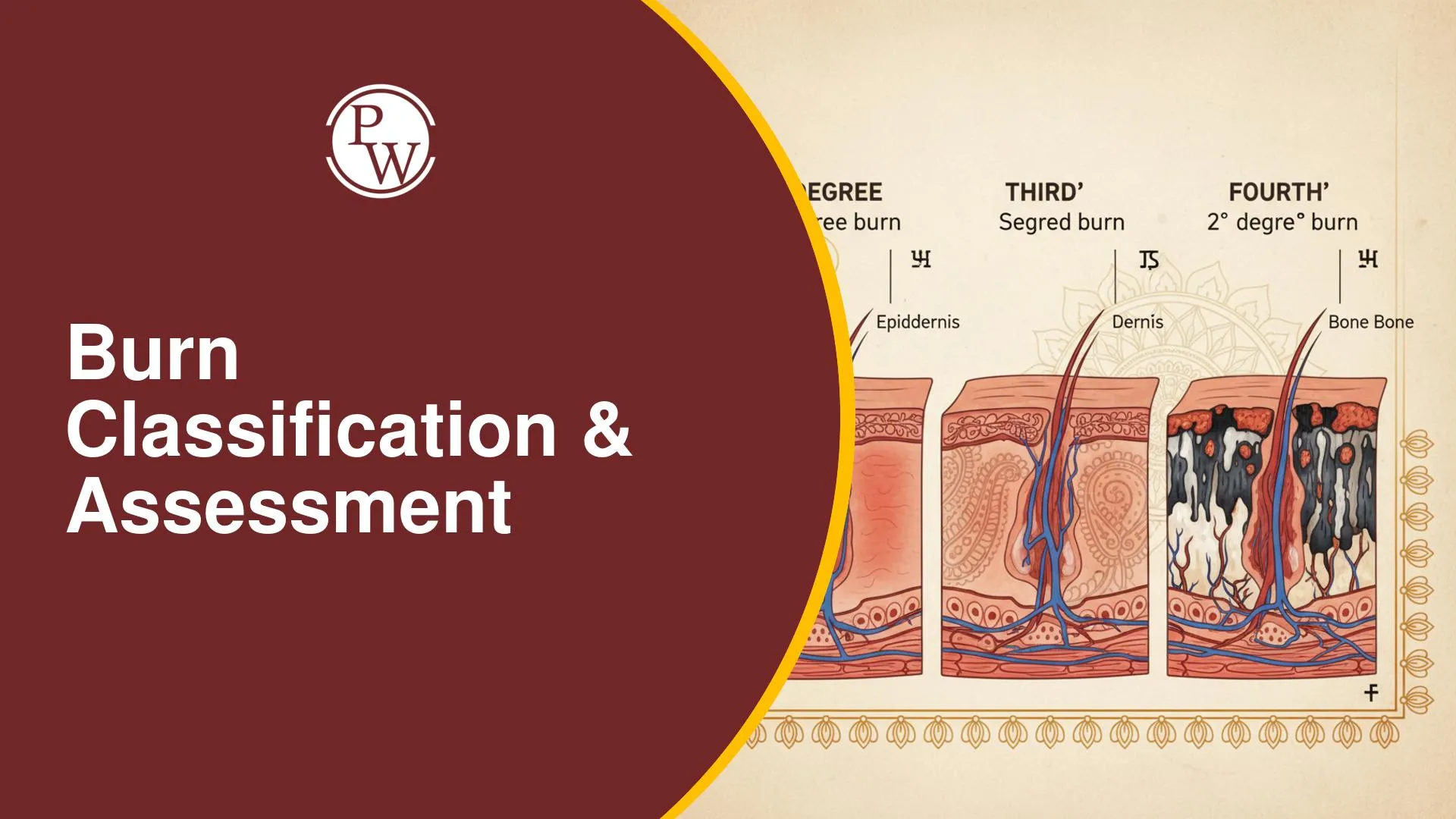
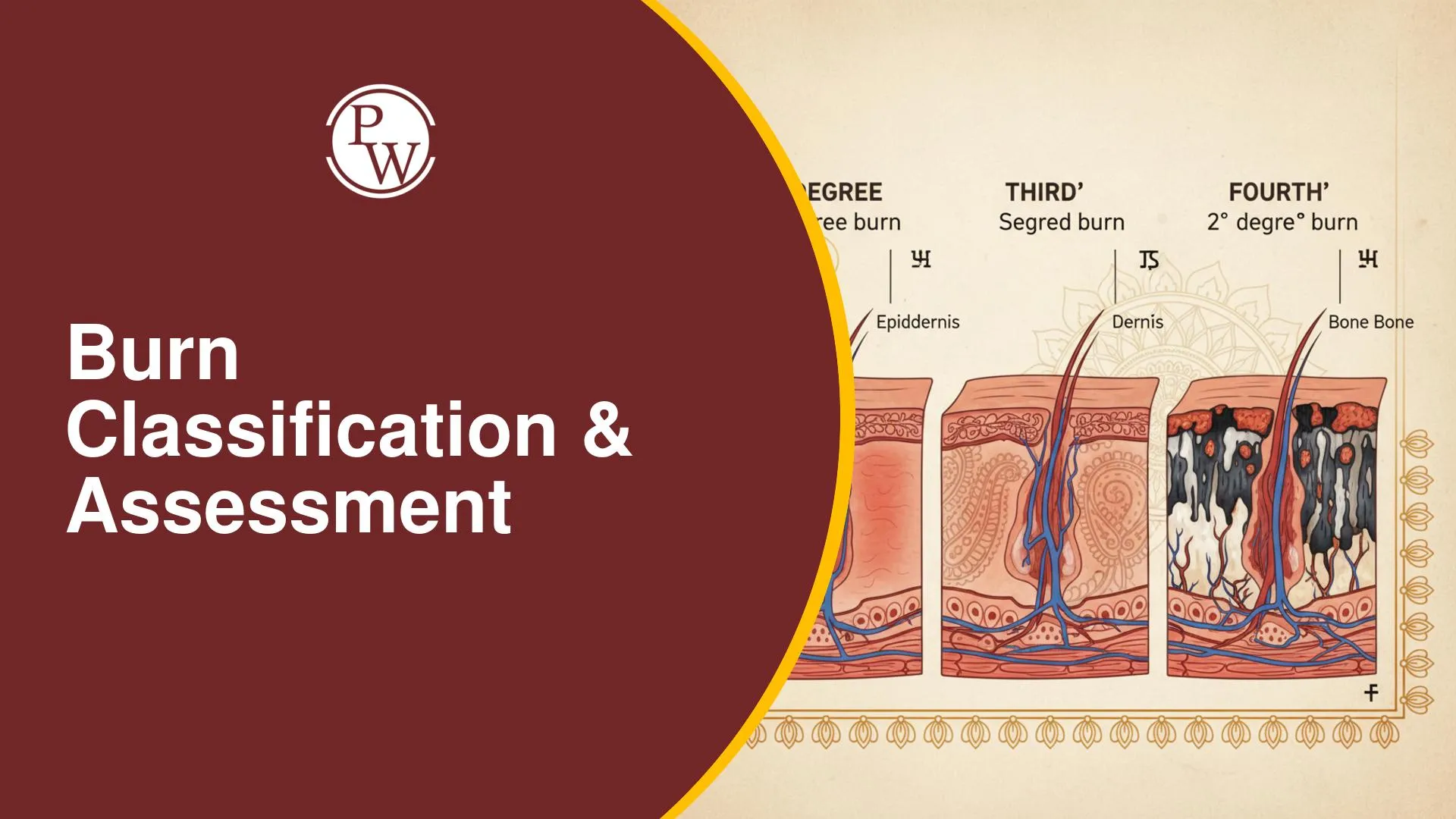
Classification of Burn Wounds by Depth
Burn wounds are classified based on their depth, which determines structures involved, symptoms, and healing potential.
|
Classification of Burn Wounds by Depth |
|||||
|---|---|---|---|---|---|
|
Classification |
Structures Involved |
Pain |
Blister |
Color |
Healing |
|
Superficial Burn |
Epidermis only |
Extremely painful |
Not seen |
Blanching erythema |
Will heal |
|
Superficial Partial Thickness Burn |
Papillary dermis |
Painful |
Characteristic (present) |
Non-blanching erythema |
Will heal |
|
Deep Partial Thickness Burn |
Reticular dermis |
No pain, but pin prick sensation |
May or may not be present |
Mottled pink appearance / Waxy white |
Will heal |
|
Full Thickness Burn |
Full thickness of skin, subcutaneous fat, underlying muscle/vessel/bone/tendon |
No pain |
No blisters |
Leathery / Charred black appearance |
Will NOT heal, requires intervention |
Summary of Initial Assessment for Burns
The initial assessment of a burn patient involves a structured approach:
-
Primary Survey: Manage ABCDE and perform immediate interventions (oxygen, IV access, tetanus prophylaxis) while monitoring for warning signs for intubation.
-
Secondary Survey: Assess TBSA burnt using rules like the Valis Rule, and manage the wound, including debridement and viable/non-viable tissue assessment.
-
Burn Wound Management: Initiate a thorough wash within 1 hour of the burn, understanding its objective, appropriate fluid, and duration.
-
Evaluate criteria for admission to a burn ward.
-
Understand the definition of significant burns (age-based and uniform).
-
Utilize Jackson's Thermal Wound Theory to understand the zones of injury.
-
Classify burn wounds based on depth using clinical criteria.
Burns Classification & Assessment FAQs
Q1: What is the primary goal of the secondary survey in burn patients?
Q2: What is the preferred fluid for initial resuscitation in significant burns?
Q3: Name two crucial immediate interventions performed during the primary survey for a burn patient.
Q4: When is a thorough wash effective for burn wounds, and what is its primary objective?
Q5: What are the three zones of injury described by Jackson's Thermal Wound Theory?

Get Free Counselling Today
and Clear up all your Doubts
