Oral Cavity Examination, Detailed Step by Step Procedure


An oral cavity examination is a fundamental part of clinical ENT and head–neck assessment. A careful, step-by-step inspection of the lips, gums, teeth, tongue, palate, floor of mouth, sulci, retromolar trigone, and oropharynx helps detect infections, inflammatory conditions, restricted mouth opening (trismus), premalignant lesions, and early oral cancers.
A systematic approach with proper illumination, patient positioning, and use of a tongue depressor allows clear visualization of important anatomical landmarks. Understanding what to inspect and why each area is clinically significant ensures accurate diagnosis and improves overall examination skills in routine ENT practice.
Also Read - NEET PG 2026
Patient Preparation and Consent for Oral Cavity Examination
Before starting the examination, ensure the patient is in a well-lighted room. Build rapport with the patient. It is crucial to obtain formal consent by clearly explaining the procedure, including the use of instruments like a tongue depressor.
Examination of Oral Cavity
Examination of the Lips
The oral cavity begins at the oral commissures, making the lips the starting point. Inspect the following anatomical structures and features of the lips:
-
Oral Commissures: Angles of the lip on both sides.
-
Vermilion Border: Demarcation line between skin and lip mucosa.
-
Upper Lip Tubercle: Small projection on the upper lip center.
-
Cupid's Bow: Central triangular shape of the upper lip.
-
Philtrum: Area above the Cupid's bow, below the nasal septum.
-
Mentolabial Fold/Crease: Fold below the lower lip.
-
Nasolabial Fold/Crease: Fold from the side of the nose to the corner of the mouth.
Internal Examination Preparations
For internal illumination, utilize a headlight. Instruct the patient to open their mouth. Use a lax tongue depressor, a vital instrument for examining the oral cavity and oropharynx.
Initial Internal Observations
Upon mouth opening, first observe the patient's breath. A foul smell, known as halitosis, can indicate issues with orodental hygiene. Next, assess mouth opening:
-
Normally, mouth opening should be more than 35 mm (interincisor distance).
-
This can be measured with a vernier caliper or a three finger assessment test. In the three finger assessment test, normally the mouth should open wide enough to accommodate three fingers (pulp of each finger typically 12-14 mm). Inability to open the mouth adequately indicates restriction or trismus.
Examination of Gums (Gingiva) and Teeth
Gently retract the buccal mucosa to visualize the oral vestibule (space above and below gums/teeth). Inspect the upper and lower gingiva and dentition for:
-
General orodental hygiene.
-
Tooth caries.
-
Tooth misalignment.
-
Missing teeth.
Examination of the Buccal Mucosa
Gently retract the buccal mucosa using a tongue depressor. Observe its color, any visible lesions, or growths. A key landmark is the opening of the parotid duct (also known as Stensen's duct), located on the upper buccal mucosa at the level of the upper second molar tooth. This area should be inspected and palpated for granulations, stenosis, or blockage.
Examination of Sulci
Gingivobuccal Sulcus: This is the potential space between the gums and the buccal mucosa, both upper and lower. Clinical Significance: This is a very common area for tobacco placement and a frequent site for hidden cancers or malignancy of the oral cavity, especially in the lower gingivobuccal sulcus. Inspect both upper and lower sulci carefully on both sides.
Gingivolabial Sulcus: This is the space between the lips (labial) and the gingiva (gums), both upper and lower, observed anteriorly.
Examination of the Oral Cavity Proper
Hard Palate and Soft Palate: The Hard Palate is in the roof of the mouth, characterized by palatine rugae (multiple folds) and a midline palatal raphe (central elevation). The Soft Palate is part of the oropharynx. The junction between the hard palate and the soft palate superiorly marks the boundary between the oral cavity and the oropharynx.
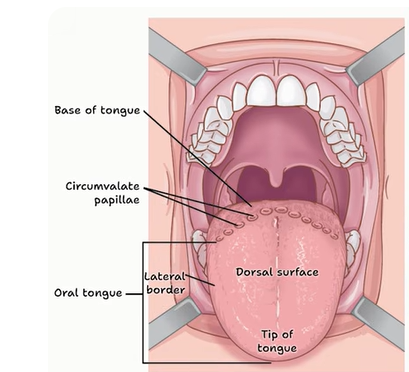
Tongue: Inspect the dorsal aspect for papillae. Also check lateral aspects for lesions. The anterior two-thirds of the tongue (the oral tongue) are part of the oral cavity. The posterior one-third (the oropharyngeal tongue or base of tongue) is part of the oropharynx. Circumvallate papillae demarcate these two parts. Clinical Note: Avoid pressing on the posterior one-third to prevent a gag reflex. Gently depress the anterior two-thirds.
On the ventral aspect, note the lingual frenulum (median fibrous band) attaching it to the floor of the mouth, prominent deep lingual veins, and Wharton's duct papillae (openings for submandibular glands).
Floor of Mouth
This area is located below the ventral aspect of the tongue and can be palpated.
Retromolar Trigone
This area is located behind the base of the third molar tooth. Clinical Significance: The retromolar trigone is a very important site and a very common malignancy site of oral cancers, often called a "coffin's corner" for ENT surgeons. It carries the maximum chances of hidden malignancies. Cancer here may necessitate a mandibulectomy during oral cancer resection.
Also Read - NEET PG 2026 Preparation
Examination of the Oropharynx
Demarcations of Oral Cavity from Oropharynx:
-
Superiorly: The junction between the hard palate and the soft palate.
-
Inferiorly: The junction between the anterior two-thirds and posterior one-third of the tongue, marked by circumvallate papillae.
Structures Visualized in the Oropharynx (after depressing the anterior two-thirds of the tongue):
-
Soft palate
-
Uvula (central hanging part)
-
Anterior Pillar: Made of the palatoglossus muscle.
-
Posterior Pillar: Made of the palatopharyngeus muscle.
-
Tonsillar Fossa: Space between the anterior and posterior pillars.
-
Tonsils: Located within the tonsillar fossa.
-
Posterior Pharyngeal Wall
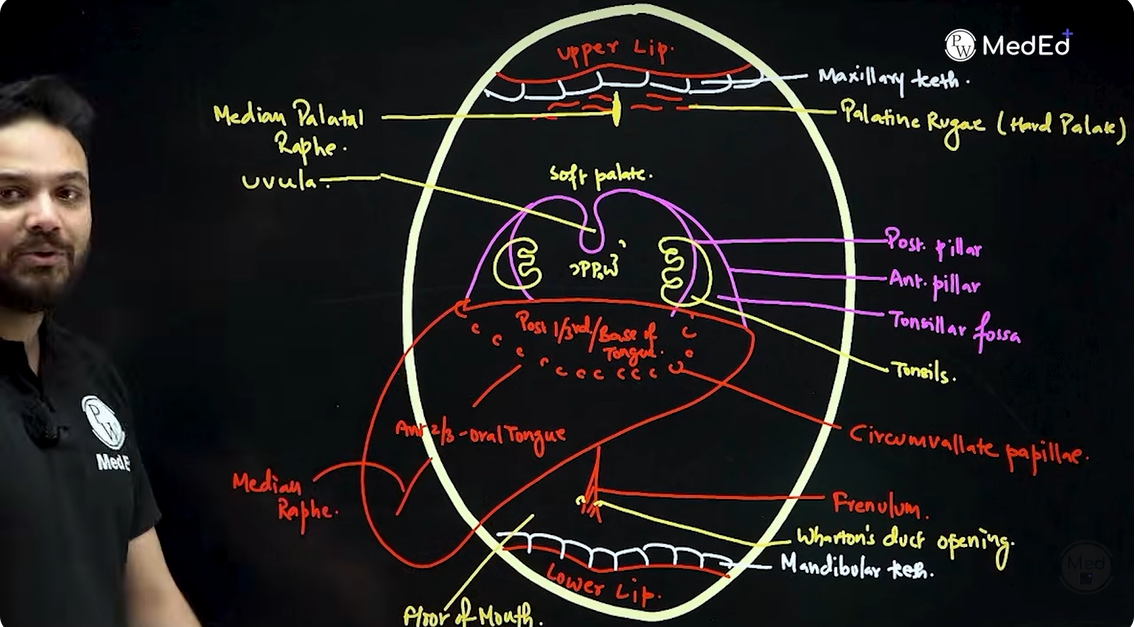
Diagrammatic Representation for Exams and Pathologies
For illustrating oral cavity and oropharynx pathologies, focus on key structures in an open mouth view:
-
Lips: Upper and lower.
-
Maxillary Teeth and Mandibular Teeth (with alveolus).
-
Oropharyngeal Structures:
-
Uvula: Central projection.
-
Anterior Pillar: Formed by the palatoglossus muscle.
-
Posterior Pillar: Formed by the palatopharyngeus muscle.
-
Tonsillar Fossa: Area between the pillars.
-
Tonsils: Within the tonsillar fossa.
-
Soft Palate.
-
Hard Palate: Showing palatine rugae and the median palatal raphe.
-
Posterior Pharyngeal Wall.
-
Tongue:
-
Anterior Two-thirds (oral tongue).
-
Circumvallate Papillae: Demarcating anterior and posterior parts.
-
Posterior One-third (base of tongue or oropharyngeal tongue).
-
Median Raphe of the Tongue.
-
Lingual Frenulum: Attaching tongue to the floor of mouth.
-
Wharton's Duct Openings: Small papillae near lingual frenulum.
-
Floor of Mouth.
Oral Cavity Examination FAQs
What are the three main segments of throat examination?
Why is the retromolar trigone considered a clinically important area?
How is normal mouth opening assessed and what indicates restriction?
Where is the parotid (Stensen's) duct opening located, and what should be inspected there?
What are the superior and inferior demarcation points separating the oral cavity from the oropharynx?