
Thyroid Anatomy & Embryology: Development, Structure & Clinical Insights
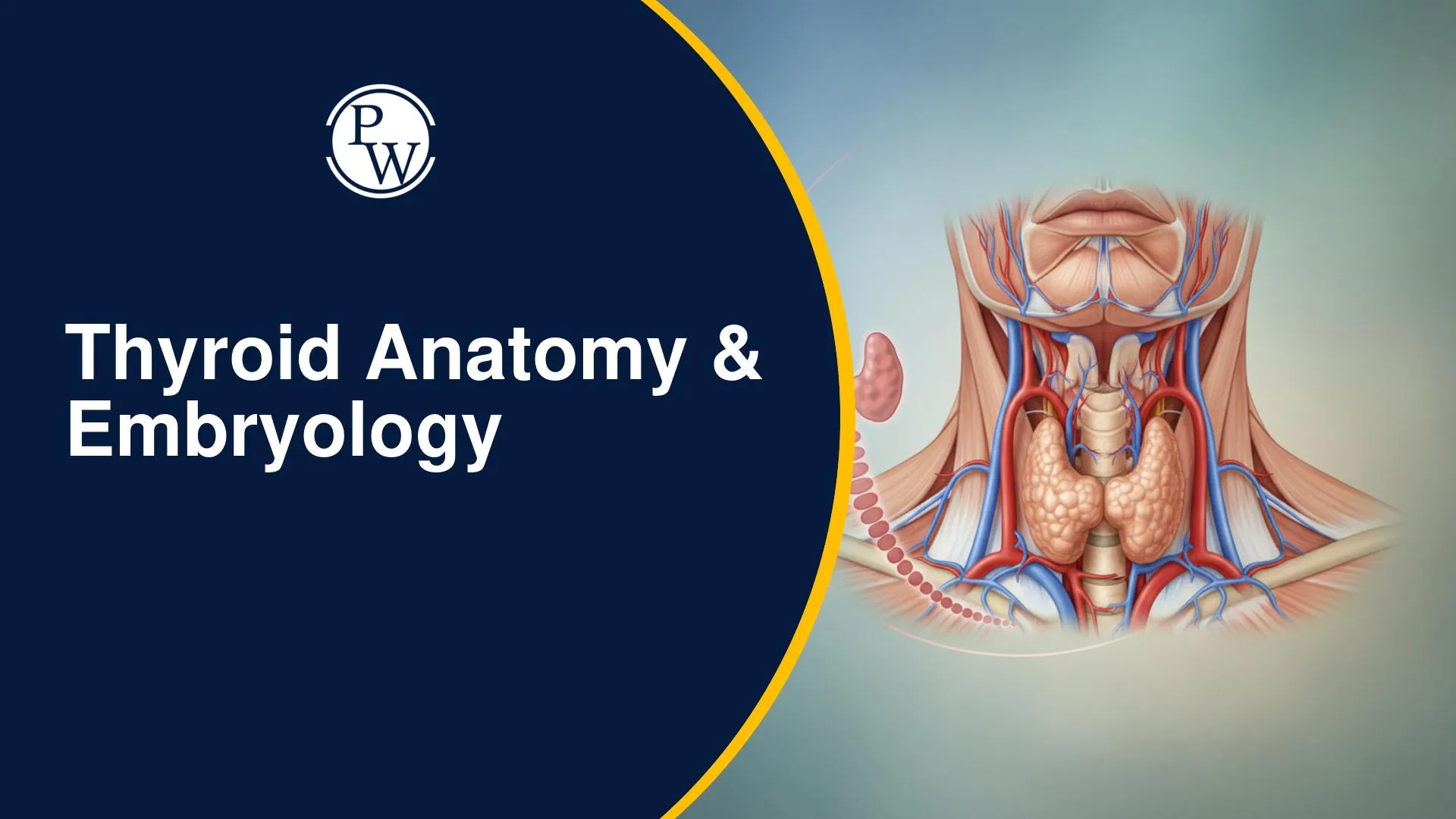
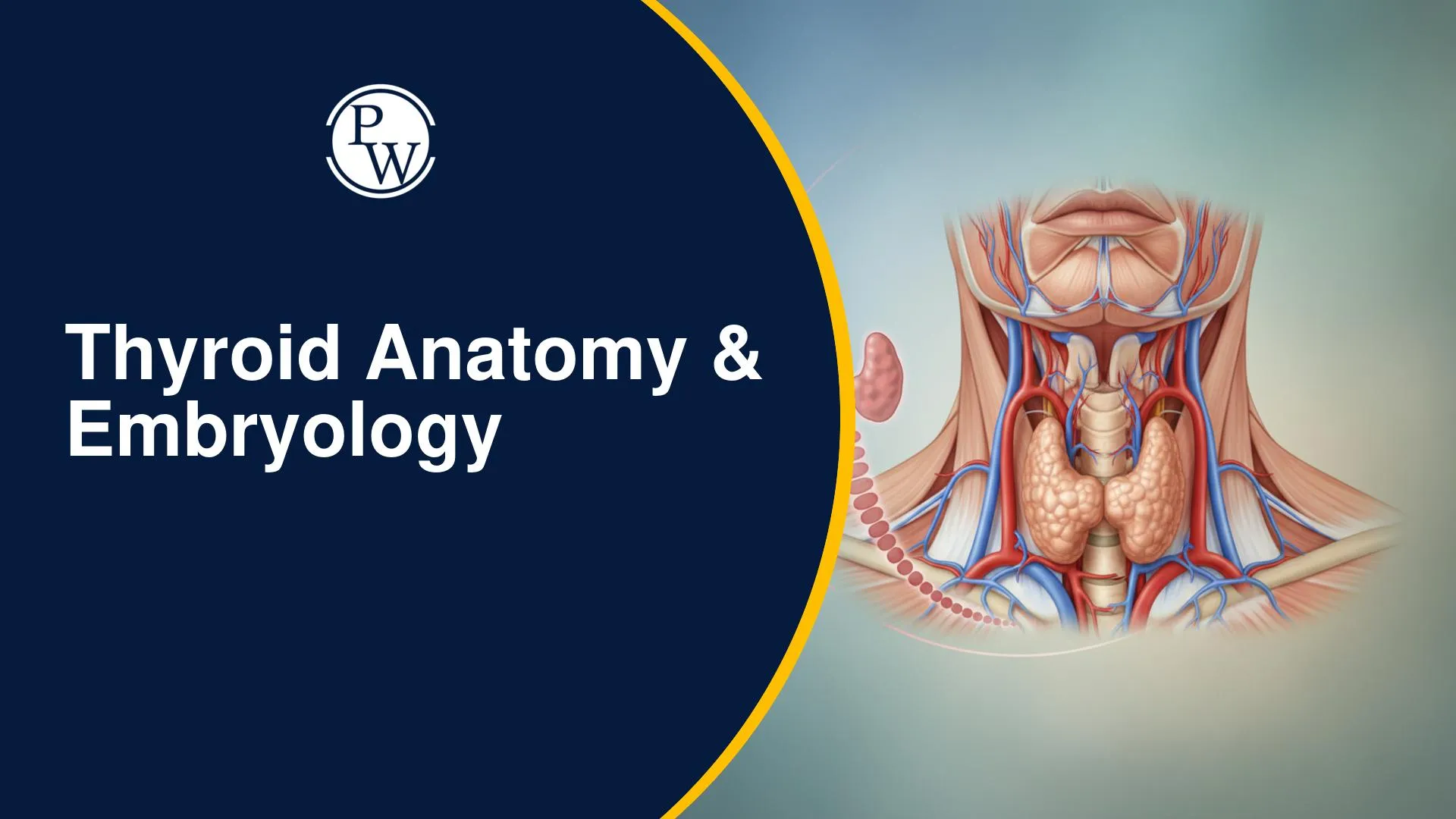
The thyroid gland is one of the most important endocrine organs in the human body, playing a central role in regulating metabolism, growth, and overall hormonal balance. A clear understanding of thyroid anatomy and embryology is essential for academic exams as well as for clinical practice, especially in surgery and management of thyroid disorders.
From its origin in the primitive foregut to its final butterfly-shaped structure in the neck, the thyroid undergoes a complex developmental process involving fusion of multiple components. Along with its structural details, knowledge of its blood supply, nerve relations, and lymphatic drainage is critical due to their direct relevance in procedures like thyroidectomy and in conditions such as thyroid malignancies.
About Thyroid Gland
The thyroid gland is a crucial endocrine organ, essential for regulating metabolism through hormone production. Check intricate development, gross and microscopic anatomy, and vital vascular, neural, and lymphatic components. Understanding these aspects is foundational for comprehending thyroid function and clinical interventions related to its disorders and surgical management.
1. Development of the Thyroid Gland
The thyroid gland originates from the primitive foregut. Its development involves several key stages:
-
Pharyngeal Arches: The process starts in the region between the first and second pharyngeal pouches.
-
Median Thyroid Diverticula: During the third week of gestation, a small median thyroid diverticula (or median bud) forms here.
-
Lateral Anlagen: Concurrently, two paired lateral anlagen emerge from the fourth pharyngeal arch.
-
Thyroglossal Duct Formation: As the embryo grows, the median diverticula elongates downwards, forming the thyroglossal duct.
-
Fusion: The thyroglossal duct descends, and the lateral anlagen move towards the midline, eventually fusing together.
-
Final Structure: This fusion culminates in the characteristic butterfly-shaped thyroid gland.
2. Gross Anatomy and Histology of the Thyroid Gland
The thyroid gland comprises:
-
Lobes: A right lobe and a left lobe.
-
Isthmus: A connecting bridge between the two lobes, known as the isthmus of the thyroid.
Comparative Structure: Thyroid Lobes
-
The right lobe of the thyroid gland is always bigger when compared to the left lobe.
Microscopic Anatomy:
-
The thyroid gland is organized into smaller units called lobules by septa.
-
Within each lobule, the functional cells are thyroid follicles.
-
Thyroid follicles are the functional unit of the thyroid gland, responsible for secreting thyroid hormones (T3 and T4).
-
Surrounding these follicles are specialized parafollicular cells (or parafollicular C cells).
-
Parafollicular C cells produce calcitonin.
Comparative Structure: Active vs. Dormant Follicles
The epithelium of thyroid follicles reflects their activity:
-
Active Follicle: Features cuboidal epithelium.
-
Dormant Follicle: Features columnar epithelium, indicating less activity in T3 and T4 secretion.
3. Extent and Surface Anatomy of the Thyroid Gland
The thyroid gland sits anterior to the trachea, with its isthmus typically covering the tracheal rings.
-
Superior-Inferior Extent: The gland's normal range is from the fifth cervical vertebra (C5) to the first thoracic vertebra (T1).
-
The superior pole reaches C5.
-
The inferior pole extends to T1.
-
Isthmus Location: The isthmus is positioned between the third and fourth tracheal rings.
4. Vascular Anatomy of the Thyroid Gland
The thyroid gland receives a dual blood supply from the superior and inferior thyroid arteries.
4.1 Arterial Supply
-
Superior Thyroid Artery:
-
This is the first branch of the external carotid artery.
-
Inferior Thyroid Artery:
-
A branch of the thyrocervical trunk, which itself stems from the subclavian artery.
-
The parathyroid glands predominantly receive their blood supply (about 80% of the time) from the inferior thyroid artery.
-
Thyroid Ima Artery (Anomalous Supply):
-
An accessory blood supply to the isthmus of the thyroid gland.
-
It originates from the brachiocephalic artery.
-
Present in approximately 30% of patients.
-
Clinical Importance: Surgeons must be extremely careful when dissecting the isthmus, particularly its inferior surface, to prevent injury to the thyroid Ima artery.
4.2 Venous Drainage
The thyroid gland is drained by three main veins:
-
Superior Thyroid Vein: Drains into the internal jugular vein.
-
Middle Thyroid Vein: Drains into the internal jugular vein.
-
Inferior Thyroid Vein:
-
The inferior thyroid veins (both right and left) drain into the left brachiocephalic vein.
5. Neural Component Associated with the Thyroid Gland
Nerves near the thyroid gland are surgically significant due to their proximity, even though they do not directly innervate the gland.
-
Vagus Nerve (CN X): Gives rise to the laryngeal nerves. (Memory Tip: In the abdomen, the left vagus nerve becomes anterior, and the right vagus nerve becomes posterior (LAP: Left Anterior, Right Posterior).)
-
Superior Laryngeal Nerve:
-
Divides into internal and external branches.
-
The external branch of the superior laryngeal nerve is closely associated with the thyroid gland.
-
Recurrent Laryngeal Nerve:
-
Follows a recurrent path back up into the neck, traveling in the tracheoesophageal groove to supply the vocal cords.
-
Left Recurrent Laryngeal Nerve: Loops through the arch of the aorta.
-
Right Recurrent Laryngeal Nerve: Loops through the right subclavian artery.
Comparative Structure: Length of Recurrent Laryngeal Nerves
-
The left recurrent laryngeal nerve is longer compared to the right recurrent laryngeal nerve due to its course around the aortic arch.
6. Lymphatics of the Neck
Understanding neck lymphatic drainage is vital for managing thyroid malignancies. Neck lymph nodes are categorized into levels:
-
Level 1a: Submental group (under the chin).
-
Level 1b: Submandibular group (below the mandible).
-
Level 2: Upper jugular group.
-
Level 2a: Anterior to the spinal accessory nerve.
-
Level 2b: Posterior to the spinal accessory nerve.
-
Level 3: Middle jugular group.
-
Level 4: Lower jugular group.
-
Level 5: Posterior triangle lymph nodes.
-
Level 5a: Along the spinal accessory nerve.
-
Level 5b: Along the transverse cervical artery.
-
Level 6: Central group of lymph nodes.
-
Clinical Importance: This level is very important for thyroid malignancies. In thyroid surgery, if involved, the Level 6 lymph nodes must be removed.
-
Level 7: Mediastinal group of lymph nodes.
Clinical Application in Neck Dissections:
-
Modified Radical Neck Dissection: Involves removing lymph nodes from Level 1 to Level 5.
-
Central Neck Dissection: Involves removing lymph nodes from only Level 6.
Thyroid Anatomy & Embryology FAQs
How does the thyroid gland develop embryologically?
What are the functional units of the thyroid gland and their secretions?
What are the primary arterial supplies to the thyroid gland?
Why is the thyroid Ima artery clinically significant?

Get Free Counselling Today
and Clear up all your Doubts
