Multiple Myeloma: Etiology, Pathophysiology
Share
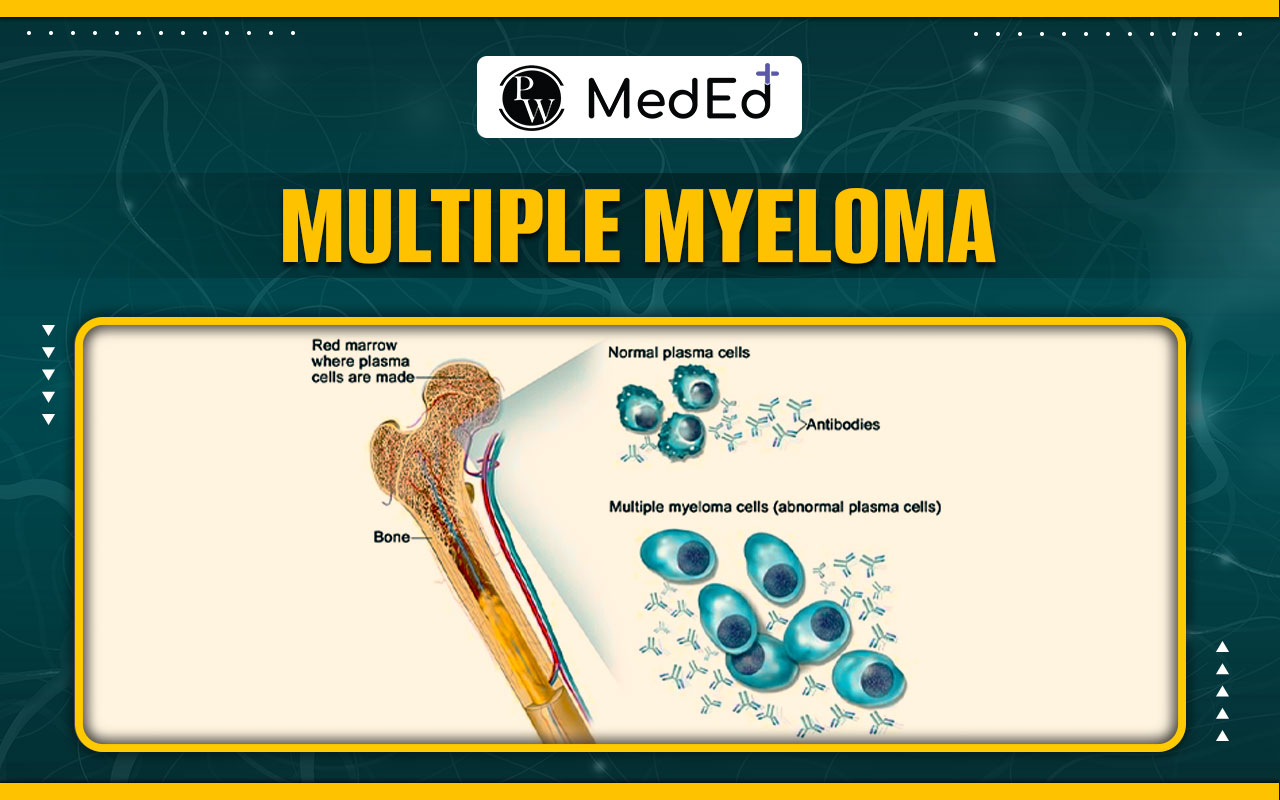
Multiple Myeloma , also termed plasma cell dyscrasia, is a malignancy originating from plasma cells, a type of leukocyte. Normally, plasma cells synthesize antibodies to combat infections. However, in multiple myeloma, abnormal plasma cells accumulate within the bone marrow. This marrow, a spongy tissue within bones, is responsible for hematopoiesis. The presence of cancerous cells displaces healthy blood cell production, leading to compromised immune function. Furthermore, instead of generating functional antibodies, these malignant cells produce defective proteins, contributing to the complications associated with multiple myeloma.
Etiology of Multiple Myeloma
- Radiation exposure, a known risk factor for most blood cancers, is implicated in the etiology of multiple myeloma.
- Occupational exposure to petrochemicals, particularly among woodworkers and farm workers, increases the risk of developing multiple myeloma.
- Genetic abnormalities such as deletion of chromosome 17p and hyperploidy at 13q14 contribute to the pathogenesis of multiple myeloma.
Pathophysiology of Multiple Myeloma
Clinical Manifestations of Multiple Myeloma
Clinical Manifestations of Multiple Myeloma can be summarized with the acronym CRAB:- C : Hypercalcemia, primarily due to lytic bone lesions, which can lead to cardiac arrhythmias.
- R : Renal failure, often secondary to hypercalcemia as a major contributor.
- A : Anemia, typically normocytic normochromic, resulting from plasma cell infiltration of the bone marrow.
- B : Bleeding tendencies and bony lytic lesions.
- Normocytic normochromic anemia occurs because plasma cells invade the bone marrow, crowding out normal hematopoietic cells.
- Bleeding tendencies arise from impaired platelet production in the crowded bone marrow or from platelet dysfunction caused by abnormal antibodies.
- Bone pain or low backache is common.
- Differential diagnosis includes ruling out osteoporosis, disc prolapse, and metastatic prostate carcinoma involving the spine.
- Spinal fractures can occur, posing a risk of paraplegia due to compressive myelopathy.
- Lethargy or fatigue due to anemia may be present.
- Renal dysfunction leads to uremia, with crystalline deposits causing uremic frost after sweating, and potentially causing asterixis and metabolic encephalopathy.
- Hyperviscosity syndrome can manifest as dizziness and vertigo.
- Amyloidosis associated with multiple myeloma can lead to carpal tunnel syndrome.
Investigations
Treatment of Multiple Myeloma
Treatment for multiple myeloma involves the following medications for the induction phase:- Steroids: Dexamethasone
- Immunomodulators: Thalidomide and lenalidomide
- Proteasome inhibitor: Bortezomib
Are you preparing to excel in the MBBS NExT Exam 2025? Access the PW Med Ed app today to study under the guidance of leading medical experts and achieve excellent scores in your exam preparation.
Multiple Myeloma NExT Exam FAQs
What is multiple myeloma?
What are the risk factors associated with multiple myeloma?
What are the common clinical manifestations of multiple myeloma?
How is multiple myeloma diagnosed?
What are the treatment options available for multiple myeloma?